Today you’re going to learn the potential benefits of marijuana.
We analyzed over 150 scientific papers to find all potential benefits of marijuana.
Some of these studies are human studies, while others are animal studies.
Keep in mind that the results of animal studies can’t be directly extended to humans. Human clinical trials with cannabis are rare. Therefore we emphasize that these are potential benefits.
Most of the potential benefits of marijuana come from cannabinoids like THC and CBD.
But marijuana also has other types of compounds with health benefits:
- terpenes, and,
- flavonoids.
Some researchers think that all these compounds work together. They think that the benefits of cannabis can’t be reduced to isolated compounds. Cannabis is a ‘synergistic shotgun’ of beneficial compounds.
But marijuana legalization has more potential benefits than health-related benefits. These benefits you’ll learn today as well.
A discussion on the benefits of marijuana wouldn’t be complete without covering the health risks.
Even though marijuana has many potential benefits…
You’ll also learn that marijuana-use comes with serious health risks. You should be careful not to abuse it.
Health Benefits of Marijuana
1. Helps relieve nausea and vomiting in some chemotherapy patients

THC is the most well-known cannabinoid inside cannabis.
Research shows that THC can be useful in relieving chemotherapy-induced nausea and vomiting.
A study done in 2001 (1) with chemotherapy patients found that:
patients who smoked cannabis showed a 70 – 100% relief from nausea and vomiting, while those who used a Δ9-THC capsule experienced 76 – 88% relief.
2. Stimulates appetite and weight gain in AIDS, cancer, and anorexia nervosa patients
Many studies show marijuana use is directly correlated with increased appetite and weight. The exact mechanism is still unclear. But we do know there’s a high concentration of cannabinoid receptors in brain parts controlling food intake.
A couple of example studies:
A 1994 study looked at the effects of marijuana on mean daily energy intake. Mean daily energy intake of participants who used marijuana was significantly higher than those that didn’t (2).
A 1988 experimental study found that smoked marijuana increased total daily caloric intake by 40% (3).
[cbdquiz]
3. Decreases spasticity associated with multiple sclerosis (MS)
The effects of marijuana on:
- psychomotor dysfunction, and,
- spasticity,
associated with multiple sclerosis are well documented.
Various studies show marijuana can decrease spasticity in multiple sclerosis patients. Especially in patients receiving insufficient relief from traditional treatments.
Especially smoking marijuana has strong evidence for decreasing spasticity and pain.
For example:
A study done in 2012 found that inhaled cannabis had a beneficial effect on spasticity among MS patients receiving insufficient relief from traditional treatments (4).
Another anecdotal example, an MS patient given CBD:
4. Could help with amyotrophic lateral sclerosis (ALS)
ALS is one of the 3 most deadly neurodegenerative diseases known to man. More research is needed, but animal studies show that cannabinoids have neuroprotective properties. Cannabinoids may counteract some of the effects of ALS.
A 2006 study looked at the effects of cannabinoid receptor 2 (CB2) activation on ALS in mice (5). Activation of the CB2 receptor resulted in better motor unit survival and motor neuron survival.
The researchers didn’t test marijuana specifically. But THC activates the CB2 receptor as well, and in theory, would have the same effects. Further research should point if that’s really the case.
5. Relieves all symptoms associated with spinal cord injury in some patients
Spinal cord injury (SPI) can be condition that interferes with your daily life. Some SPI symptoms that particularly can interfere with your general well-being are:
- pain,
- muscle spasms,
- spasticity, and,
- difficulties sleeping.
At least one study shows that it can also improve general quality of life in spinal cord injury patients (6).
6. Can help with epilepsy
Studies suggest that epileptic activity is related to changes in:
- the levels, and,
- distribution,
of cannabinoid receptors in the hippocampus.
So it’s no coincidence that for decades, cannabinoids are used to reduce seizures. Cannabinoids are especially popular with patients that have a resistance to traditional treatments (7).
7. Could alleviate chronic pain
Chronic pain is a complex condition that involves many factors and is a cause of reduced quality of life.
Clinical studies show that smoked or vaporized marijuana can decrease chronic neuropathic pain. Chronic neuropathic pain is a symptom of various syndromes and diseases.
For example:
A 2011 study looked at the effects of vaporized marijuana on chronic neuropathic pain. Vaping cannabis 3 times a day for 5 days resulted in a significant decrease (27%) of perceived pain in chronic pain patients (8).
8. May help treat bladder pain syndrome (BPS)
BPS can keep you up all night forcing you to frequent the bathroom at rather unwanted times.
In 2014 researchers found that activation of cannabinoid receptor 2 (CB2), decreased:
- bladder inflammation, and,
- urinary frequency,
in mice with BPS (9).
This same cannabinoid receptor gets activated by THC. THC is one of the main cannabinoids in marijuana. In theory, this means that marijuana has the potential to help with BPS. Further research is needed to explore this potential.
9. Reduces headaches and migraine attacks in some patients
Heavy migraines can be debilitating.
I have 2 friends who suffer heavily from migraines from time to time and marijuana helps them tremendously in coping with it.
Research shows that activation of the endocannabinoid system (10):
could represent a promising therapeutical tool for reducing both the physiological and inflammatory components of pain that are likely involved in migraine attacks
The cannabinoids inside marijuana are some of the most potent activators of the endocannabinoid system. As you can see, anecdotal reports are slowly starting to get back up from scientific research.
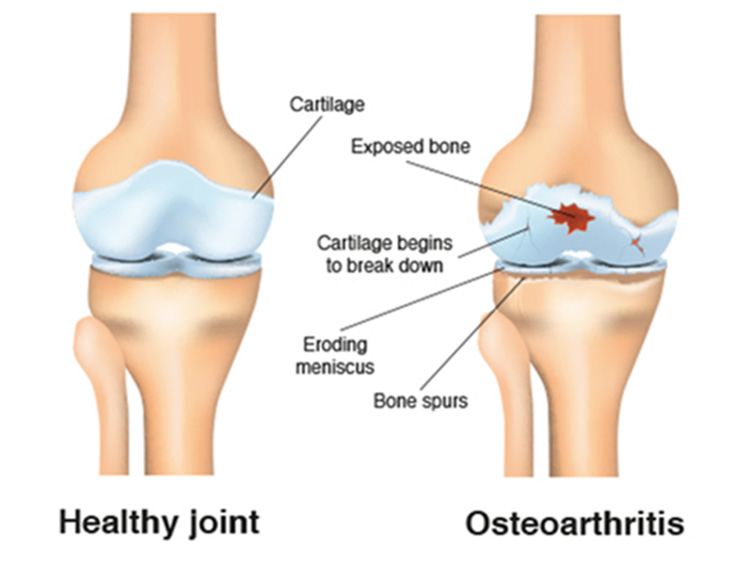
10. Could help with osteoarthritis (OA) by preventing cartilage breakdown
Research on this topic is scarce. But some animal studies show activation of cannabinoid receptors helps control pain caused by OA (11).
A more recent human study looked at the effects of CB2-receptor activation on cartilage breakdown in OA (12). The study concluded that:
cannabinoids may prevent cartilage breakdown in OA.
11. Could relieve rheumatoid arthritis pain and stop its progress
Again the research on this topic is scarce, but the research that has been done is promising.
Unlike OA, rheumatoid arthritis is an autoimmune disease where the immune system attacks your joints.
Marijuana-based medicines could help with relieving pain caused by rheumatoid arthritis.
For example:
A 2005 study found that a cannabis-based medicine named Sativex had pain-relieving effects in RA patients (13). Sativex also suppressed the disease activity of rheumatoid arthritis in patients.
12. Can help with all symptoms associated with fibromyalgia
Fibromyalgia is a chronic pain condition that can affect your daily life through:
- fatigue, and,
- cognitive and emotional disturbances.
Although nothing suggests that marijuana could cure fibromyalgia, a growing body of evidence shows that marijuana could help with treating its symptoms.
For example:
A 2011 study found that fibromyalgia patients that used cannabis, showed (14):
- a significant reduction in stiffness and pain,
- enhancement of relaxation, and,
- a general increase in feelings of well-being.
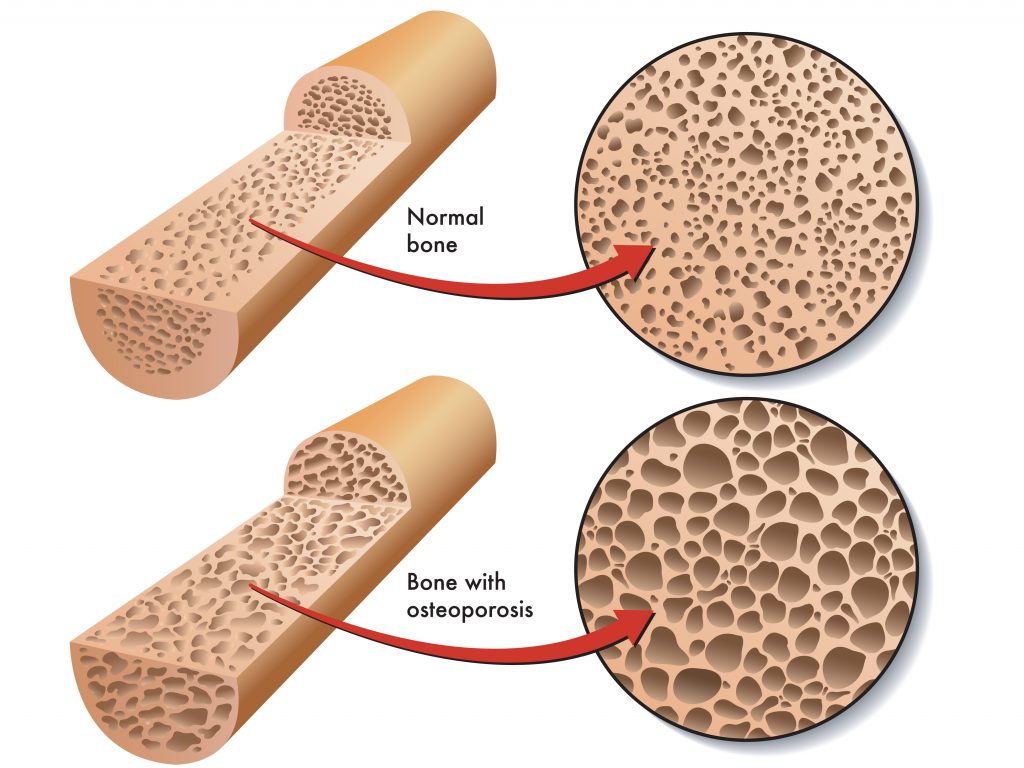
13. Could help with osteoporosis by stimulating bone formation
Osteoporosis is a bone disease that increases the risk of fractures. It causes a reduction in bone mineral density.
Cannabinoid receptor 2 (CB2) stimulates bone formation and inhibit bone resorption. This receptor gets activated by cannabinoids found in marijuana (especially THC).
A 2009 study concluded that research points towards a potential role for cannabinoid drugs to combat osteoporosis (15).
14. Could prevent degenerative disc disease (DDD)
Degenerative disc disease is the degeneration of intervertebral discs located in the spine. It can lead to severe and chronic neck and back pains.
A 2014 rat study found that repeated injection of CBD improved DDD symptoms even 15 days after CBD injection was stopped (16).
CBD is a cannabinoid widely found in cannabis.
15. Can improve symptoms associated with dystonia up to 50%
Dystonia is a neurological movement disorder that causes abnormal movements and muscle contractions.
A 1986 study found that daily intake of 100mg to 600mg of CBD co-administered with standard medication, improved dystonia up to 50% (17).
This is quite a massive improvement. It warrants a deeper exploration of the potential benefits that marijuana has for dystonia patients.
16. Could weaken the progression of Huntington’s disease (HD)
HD is a genetic neurodegenerative disease that results in the progressive loss of brain cells. As the disease progresses, it results in problems with:
- mood,
- mental abilities, and,
- psychomotor abilities.
One clinical study that looked at the efficacy of CBD on improving symptoms related to HD found no significant effect.
But a study done in 2010 concluded that downregulation of cannabinoid receptor 1 is a key pathogenic effect in HD. Activation of this receptor might weaken the progression of HD (18).
The cannabinoids in marijuana activate the CB1 receptor. Further research should show whether marijuana has any potential for helping with HD.
17. Helps with the movement disorders associated with Parkinson’s disease (PD)
PD is another neurodegenerative disease that mainly affects the motor system.
A 2001 study found that marijuana decreases tremors associated with levodopa-induced movement disorders (19). Levodopa is one of the main medications used to treat PD.
Anecdotal evidence, a PD patient treating his tremors with marijuana:
18. Helps with Tourette’s syndrome (TS)
TS is an inherited neuropsychiatric disorder characterized by physical and vocal tics.
Like with many inherited disorders there’s no cure for TS. But a 2014 study found that THC can cause a significant tic reduction in TS patients (20).
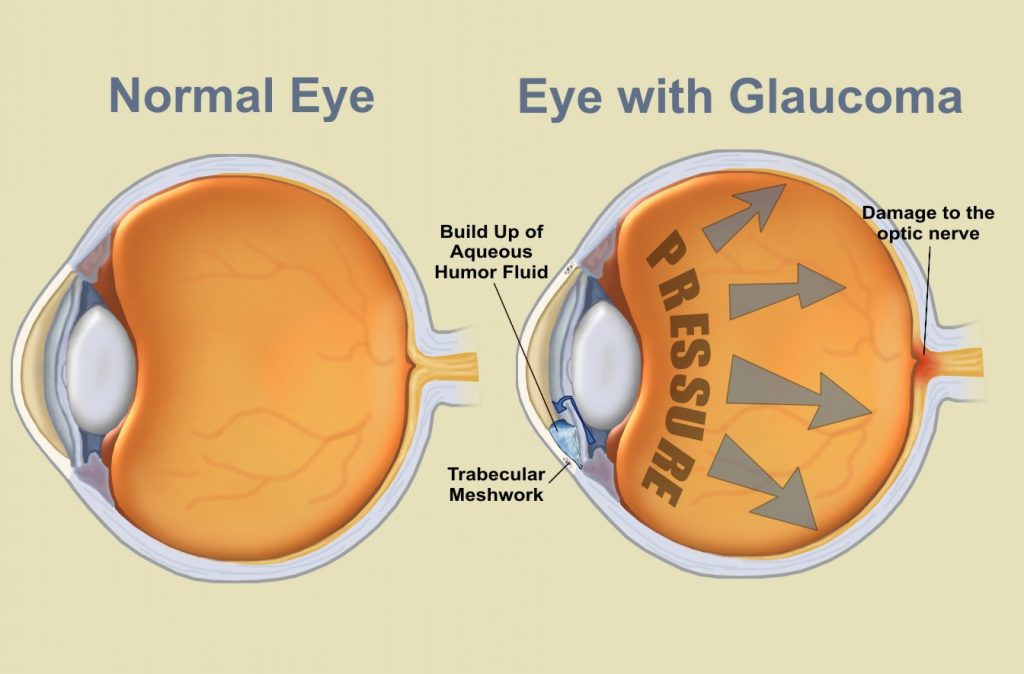
19. Could help with glaucoma
Glaucoma is an eye disease that can ultimately lead to irreversible blindness.
A study done in 2004 that analyzed different research papers concluded that because:
- cannabinoids lower intraocular pressure (one of the main risk factors in glaucoma), and,
- have neuroprotective effects,
cannabinoids could be useful in the treatment of glaucoma (21).
20. Acts as a bronchial dilator in asthma patients
The main cannabinoid in marijuana, THC, improves ventilatory function in asthma patients (22).
However, smoking is not the best idea for health, especially for an asthma patient because it can irritate and damage the delicate respiratory system.
But smoking isn’t the best idea for health. Especially for an asthma patient. Because it can irritate and damage the delicate respiratory system.
Instead, if you have asthma and want to use marijuana, use a dry herb vaporizer.
21. Can lower arterial blood pressure in patients with hypertension
Hypertension or high blood pressure is one of the major risk factors for all kinds of diseases. Mainly diseases related to the heart and arteries.
We all heard marijuana can calm you down, but did you know it can also calm down your blood pressure?
A 1979 study found that THC decreases arterial blood pressure in hypertensive subjects (23).
22. Can reduce anxiety
One side effect of THC is anxiety. But a 2011 study with social anxiety patients found that CBD reduces (24):
- anxiety,
- cognitive impairment,
- discomfort in speech performance, and,
- alert in anticipatory speech.
Important here to note is that most marijuana strains are very low on CBD. So if you would want this effect you need to get a high-CBD strain.
23. Can be an effective anti-depressant
Depression is a complex mental problem, and should always be treated by looking at the deeper underlying causes.
However if you’re depressed options can run short, and a temporary boost in mood can lead to mental clarity which can, in turn, lead to different perspectives on the causes of your depression.
In 2007 researchers found that at low doses, THC acts as an effective anti-depressant. It increases activity of the feel-good neurotransmitter in your brain: serotonin (25).
But there’s a catch:
At higher doses, THC had the opposite effect and increased feelings of depression. So don’t go blindly using marijuana to treat your depression. Always consult with your doctor before going on a path of self-medication.
24. Can help with sleep disorders by effectively improving sleep quality
Anyone that ever used marijuana before going to bed knows how easy it can be to fall asleep after a good session.
But did you know cannabis and its derived medicines are prescribed for people with sleep disorders?
For example:
In 2007, researchers found that Sativex improved sleep parameters in pain patients (26). The study included 1000 patients suffering from various pain conditions. Of all patients, 40–50% attained:
good or very good sleep quality, a key source of disability in chronic pain syndromes that may contribute to patients’ quality of life.
25. Can help eliminate nightmares associated with PTSD
PTSD can be an extremely impactful mental disorder, which develops after a person experiences a traumatic event.
For example:
2009 research with PTSD patients found that a cannabis-based medicine named nabilone (27):
- reduced daytime flashbacks, and,
- improved sleep quality.

26. Can be used to control the abuse of more harmful drugs
Although marijuana use can be harmful to your health, in some cases of drug abuse, it can function as a harm-reduction tool, by taking the place of the harmful drug that’s being abused.
Researchers who surveyed 350 medical cannabis patients found that (28):
- 40% reported using medical marijuana as an alternative for alcohol,
- 26% as a substitute for illicit drugs, and,
- 66% as an alternative for prescription drugs.
The main reasons for using medical marijuana as a substitute were found to be:
- Less adverse side-effects, and;
- Better symptom management.
Be careful here though. Depending on how often and how much you use marijuana, it could be as harmful to your health as abusing other drugs.
27. CBD is a potent antipsychotic for schizophrenia patients
Marijuana use is linked to the development of schizophrenia and psychosis in persons with a susceptibility towards psychiatric disorders.
Marijuana use is linked to the development of schizophrenia and psychosis in persons with a susceptibility towards psychiatric disorders.
But what most people don’t know is that CBD, the second most well-known cannabinoid in marijuana, is a very potent antipsychotic.
A 2012 study shows that CBD is as potent an antipsychotic as one of the most used medicines in the treatment of schizophrenia, amisulpride (29).
The best part?
CBD had fewer negative side effects than amisulpride.
To get the benefits of CBD, we recommend getting a high-quality CBD oil.
28. Could help with Alzheimer’s disease (AD) and dementia
AD is a neurodegenerative disease that can eventually lead to dementia.
One of the key processes which lead to the loss of brain cells in Alzheimer’s disease is amyloid or Aβ aggregation.
THC is a very effective inhibitor of Aβ aggregation (30). In this study, THC was even more effective as an inhibitor of Aβ aggregation than the currently approved prescription drugs for AD.
29. Could help with inflammatory skin diseases
One study found a positive effect of the synthetic cannabinoid “HU-210” on pain and irritation that comes with skin inflammation (31).
Important to note here is that HU-210 is 100 to 800 times more potent than natural THC. Further research should show how effective THC is for inflammatory skin diseases.
30. Can help with irritable bowel syndrome (IBS)
Dronabinol is a cannabis-based medicine. It’s a purified form of THC.
Dronabinol showed benefits for IBS patients with constipation and diarrhea (32).

31. Can improve symptoms of inflammatory bowel diseases
Marijuana has anti-inflammatory properties, and these properties even extend to your guts.
In 2011 researchers found that 21 out of 30 patients improved their Crohn’s disease (CD) with cannabis use (33). Also, the need for regular medications was reduced . Lastly, the frequency of surgery required went down in the years of cannabis use.
32. Can help with diseases of the liver
Did you know marijuana can help with alcohol-caused liver diseases like liver fibrosis?
The irony here is that alcohol is legal and marijuana is still illegal in large parts of the world.
In 2011 researchers found that CBD induces the death of hepatic stellate cells (34). These cells are a major cause of the development and progression of liver fibrosis. The researchers propose that CBD could be a therapeutic agent for the treatment of liver fibrosis.
33. Could help weight loss in obesity
We already know that marijuana can help with gaining weight in:
- AIDS,
- cancer, and,
- anorexia nervosa patients.
However, marijuana could help with weight loss as well. The right combination and ratios of cannabinoids could help obese persons lose weight.
A 2012 study done on rats, found that a cannabis extract with THC, CBN, CBD in a ratio of 1.0:0.2:0.4, caused a significant reduction of weight gain in obese rats (35).
34. Could potentially prevent diabetes
In 2011 researchers looked at the association between diabetes mellitus (DM) and marijuana use.
What they found was extremely encouraging:
Marijuana use was associated with a significantly lower occurrence of DM (36).
This does not mean marijuana prevents DM. But a finding like this definitely should encourage more research into this topic.
35. Can kill brain tumors
Maybe you heard of anecdotal reports describing cannabis oil treating cancers. Scientific proof of marijuana killing cancer in human patients is scarce at best.
In 2014, researchers proved that THC and CBD stop the growth of one of the most aggressive cancers: glioma (37). Especially combined with radiotherapy, THC and CBD were extremely effective in destroying glioma.
36. Could inhibit tumor growth in breast cancers
CBD just seems to have an anti-effect against any tumor type. In 2015, researchers showed that CBD inhibits tumor growth in one of the most aggressive breast cancers: triple-negative breast cancer (38). They propose that CBD could be a new therapeutic option in treating breast cancers in general.
37. Could inhibit tumor growth in melanoma
Melanoma is the most aggressive form of skin cancer.
In 2013 researchers looked at the anti-cancer properties of anandamide, which is an endocannabinoid. Endocannabinoids are compounds that are naturally produced by the body and closely resemble the cannabinoids found in marijuana.
The study found that anandamide had anti-tumor properties in melanoma by activation of CB1 receptors (39). CB1 receptors are the same receptors that get activated by THC.
So no conclusions, but definitely food for further research.
38. Could help prevent bladder cancer
An analysis of a survey with 84000 men aged 45-69, showed that cannabis users had 45% less chance of bladder cancer (40). This does not mean there’s a causal effect, but it does warrant further exploration of the topic.
Important to note here is that cannabis users who also used tobacco actually had an increased risk of developing bladder cancer.
Another reason to stop smoking cigarettes or weed mixed with tobacco.
39. Marijuana could help kill leukemia cells
Leukemia is a type of cancer of the bone marrow and blood cells. It’s the most common cancer in children.
In 2013, researchers found that cannabinoids inhibit growth of leukemia cells. They were even more effective when used in combination with one another (41).
Especially CBD and CBG combined seemed to be synergetic. This combination was the most effective in inhibiting the growth of leukemia cells.
40. May be useful against lung cancer
The body has natural defense mechanisms vs. cancer. One of them are lymphokine-activated killer (LAK) cells. These cells help kill tumor cells in the lung.
As it turns out, CBD and THC increases the susceptibility of cancer cells being killed by these LAK cells (42).
So not only does CBD directly inhibit the growth of tumor cells, but it also helps the body fight tumor cells with its own immune system.

41. Could be useful against pancreatic cancer
A 2006 study found that cannabinoids reduced growth of tumor cells in animals with pancreatic cancer (43).
Not only that but it also stopped the spreading of the tumor cells in the body.
42. Could be useful against colon cancer
More and more evidence shows that cannabinoids can help with every type of cancer.
In 2011 Italian researchers looked at the effects of CBD on colon cancer. They concluded that CBD reduced polyps, tumors, and protected DNA from oxidative damage in mice with colon cancer (44).
43. Can aid in stopping the spread of prostate cancer
A 2009 study published in the “British Journal of Cancer” found that a synthetic compound that activates the CB2 receptor inhibits the growth of prostate cancer cells in mice (45). This compound’s name is JWH-015.
This same CB2 receptor gets activated by the cannabinoids found in marijuana. THC and CBD specifically.
44. Can help with obsessive-compulsive disorder (OCD)
 A study done in 2013 looked at the effects of cannabinoid CBD on compulsive behaviors in rats. They found that CBD decreased compulsive behavior of marble-burying in OCD rats (46).
A study done in 2013 looked at the effects of cannabinoid CBD on compulsive behaviors in rats. They found that CBD decreased compulsive behavior of marble-burying in OCD rats (46).
Further research has to point out whether it can help humans with OCD.
45. Could help with atherosclerosis
Atherosclerosis is a disease in which the artery walls thicken. Over the years can lead to the obstruction of proper blood flow.
A study done in 2012 found that inhalation of marijuana could actually lead to the worsening of coronary syndromes.
But marijuana used in any other way (edibles for example) could have a healing effect on atherosclerosis (47).
46. Could aid neurogenesis
 Neurogenesis is the process by which new brain cells (neurons) are created in the brain.
Neurogenesis is the process by which new brain cells (neurons) are created in the brain.
A 2013 Brazilian study found that CBD aided neurogenesis, especially in the hippocampus. But this was in mice (48).
Further research has to conclude whether the same holds for humans.
47. Can prevent brain damage after strokes and trauma
In 2014, researchers found that if you have low amounts of THC in your system, you have 80% less chance to die from head injuries (49).
48. Can improve concentration, sleep and reduce impulsivity in ADHD patients
There are plenty of anecdotal reports of ADHD patients successfully self-medicating with marijuana.
However, science didn’t dive deeper into this topic until 2015. This was when German researchers looked at the effectiveness of marijuana in treating ADHD symptoms in 30 patients. They concluded that ALL patients improved on concentration, sleep, and impulsivity (50).
49. Could protect the brain from stress
There are plenty of anecdotal reports of marijuana helping people to cope with stress.
But is there any scientific basis backing these anecdotal reports up?
Synthetic cannabinoids help combat cognitive deficits caused by chronic stress (51).
The results of this research don’t directly extend to humans. But there seems to be some scientific basis for all the anecdotes.
50. Could help with chronic heart failure (CHF)
We already know marijuana can help lower blood pressure in persons with hypertension.
But can it also help with any heart conditions?
A study done in 2013 found that the activation of the CB1 receptor (a cannabinoid receptor) had a protective effect against CHF, in mice (52).
You must know by now how the CB1 receptor gets activated (THC).

51. Could help with malaria
Cerebral malaria is a dangerous parasitic disease that’s transmitted from mosquitoes to humans. In the most severe cases it can lead to coma or even death.
Yet, in 2015 researchers showed that one of the main medicines to treat malaria: Artesunate, was more effective when used together with CBD (53). Mice that were treated with both artesunate and CBD had full cognitive functions restored. Whereas mice that were only treated with Artesunate kept some cognitive deficits.
Even without Artesunate, mice treated with only CBD had decreases in:
- inflammation,
- anxiety, and,
- cognitive deficits.
52. Can help increase libido both in males and females
If you’ve ever used marijuana while making love, you know how it can improve your sex-life. Marijuana can increase your sensitivity to touch in almost orgasmic ways.
But did you know it also can increase your libido?
In 1987 researchers concluded that marijuana initially increases libido and potency (54). But be careful, heavy chronic use may lead to a decrease of libido.
A more recent survey with women showed that 65% of cannabis users reported cannabis-use before sex made it more enjoyable (55).
53. THC reduces the infectivity of the herpes virus
Once you’re infected with the herpes virus there, unfortunately, there’s no cure. It can lead to blisters and is even associated with certain types of cancers.
A study done in 1991 found that THC had the potential to reduce the infectivity of herpes simplex virus up to 80% (56).
Even though once herpes is in your body, there’s no way to get it out, marijuana could help prevent the infections caused by it.
Non-Health-Related Benefits of Marijuana
54. Can lead to general feelings of euphoria and relaxation
A review study found that two of the most reported feelings under the influence of marijuana were (57):
- euphoria, and,
- relaxation.
55. Legalization may be related to a decrease in traffic fatalities
While you should never drive under the influence of marijuana under any circumstance…
In 2013, researchers found that legalization of medical marijuana was related to a 10% decrease in traffic fatalities. This was the first full year after the legalization came into effect (58).
Although a possible explanation for this decrease might have to do with marijuana being a substitute for alcohol…
It doesn’t mean that driving under the influence of marijuana is safer than under alcohol.
56. Legalization may be related to reductions in rates of homicide and assault
I don’t know about you, but I don’t need any science to believe criminalizing anything that has demand in society breeds more criminality. Demand will always be met with supply. It’s simple economics.
So to me, it’s only logical decriminalizing marijuana reduces crime rates. Well, it turns out there’s scientific evidence pointing towards precisely this.
A study done in 2014 found that medical marijuana legalization was not related to increased crime rates of any type. It was related to reductions in rates of homicide and assault (59).

57. Can improve creativity
Some artists claim their creativity is better when under the influence of marijuana.
For me, this creativity finds expression in strategy games. I often come up with the wildest strategies when I’m under the influence of marijuana.
But there’s actually scientific proof besides the anecdotal evidence…
In 2014 researchers looked at different measures of creativity for:
- ex-MDMA users,
- ex-cannabis users, and,
- nondrug-users.
They found that ex-cannabis users had way more rare-creative responses than both other groups (60).
58. You cannot overdose on marijuana
Did you ever hear of anyone dying from a marijuana overdose?
Probably not. Because it’s virtually impossible.
A 2015 study looked at the ratio between the overdose benchmark and the estimated human intake of various ‘drugs’. The study found that with marijuana you would have to take more than 10.000 times the estimated human intake to overdose on it (61).
Good luck with doing that.
Some other ‘drugs’ like alcohol and nicotine were extremely high-risk in this area. Taking less than 10 times the estimated human intake can already lead to a fatal overdose with both alcohol and nicotine.
The irony is that these ‘drugs’ are legal all over the world.
59. CBD could help you stop smoking
CBD can help you quit smoking cigarettes.
In 2013, researchers let smokers who wanted quit, use a CBD inhaler whenever they had the urge to smoke. Inhaling CBD reduced the number of cigarettes they smoked by 40% (62).

60. Regulating marijuana results in massive revenue and savings for states and countries alike
A 2012 analysis in Colorado, found that regulating marijuana like alcohol would generate $60 million a year in revenue and savings (63).
This money could go into beneficial projects, and could generate thousands of new jobs.
61. Legalizing marijuana can lead to socio-economic improvements in disadvantaged communities
Prohibition of marijuana has disproportional effects on communities that already have disadvantages (64). Marijuana-offenders behind bars largely are young adults from disadvantaged communities.
Decriminalizing marijuana could promote upward social mobility. How? By giving these and future offenders a new chance to do something meaningful for themselves and their communities.
Conclusion
Research on the medical benefits of marijuana is still underdeveloped. Marijuana is officially a medicine for only a handful of conditions.
But evidence shows that the compounds inside marijuana could help with treatment of over 50 medical conditions.
Marijuana, however, isn’t only beneficial for your health. Like with every substance, it has to be used very carefully and responsibly to get the benefits.
Improper and irresponsible use of marijuana can turn it into a poison. If you abuse marijuana, you increase your risk of:
- mood disorders, and,
- long-term impairment of cognitive skills.
If you want to learn all effects that marijuana has on the brain, read our guide on marijuana’s effect on the brain.
What are the most important tips for responsible marijuana use?
- Don’t ever use marijuana if you’re under 18 years old;
- Unless you have a medical condition and your doctor prescribed you marijuana, re-consider why you want to use marijuana and try to see if there are alternatives which might give you similar effects, without any negative side-effects (think meditation, yoga, etc.);
- Unless you have a medical condition and your doctor prescribed it to you, don’t use marijuana daily and/or heavily;
- Find out if you’re susceptible to psychotic disorders. If you find out that you are, or you think you might be, don’t use marijuana. Or find strains that contain little THC and a lot of CBD;
- Since THC is what causes the ‘high’, growers have been increasing THC-percentages of their plants to unnatural levels. I would advise finding strains that have a more balanced THC/CBD ratio and are grown in an organic way.
What is the best way to use marijuana?
We believe vaping marijuana is the most convenient and safest way to use marijuana. And for that, you’ll need a dry herb vaporizer.
Marijuana smoke is harmful to your respiratory system.
Edibles can be very tricky to dose. They can hit like a truck and are somewhat unpredictable.
If you want to experiment with CBD, go to our list of CBD oils.
The three main reasons to use CBD oil are:
- pain relief,
- anxiety/stress relief,
- improved sleep.
CBD oil can be a good substitute for marijuana.
Is every type of marijuana the same?
The ONLY way you really know, what it is you’re exactly smoking, vaping or eating, is to grow it yourself.
Heavy use of pesticides and other chemical substances to ‘aid’ the growing process is common in the marijuana industry.
If you grow your marijuana yourself (of course only if it’s legal where you live), you will be 100% sure what it exactly is you’re using.
You could even opt to go for a full organic grow.
For more on growing marijuana, check out our growing supplies guide and how to grow guide.
Lastly…
If you enjoyed this article, please share this post to spread this timeless marijuana knowledge.
Scientific References:
- Musty, R. E., & Rossi, R. (2001). Effects of Smoked Cannabis and Oral δ9-Tetrahydrocannabinol on Nausea and Emesis After Cancer Chemotherapy. Journal of Cannabis Therapeutics, 1(1), 29–56. https://doi.org/10.1300/j175v01n01_03
- Mattes, R. D., Engelman, K., Shaw, L. M., & Elsohly, M. A. (1994). Cannabinoids and appetite stimulation. Pharmacology Biochemistry and Behavior, 49(1), 187–195. https://doi.org/10.1016/0091-3057(94)90475-8
- Foltin, R. W., Fischman, M. W., & Byrne, M. F. (1988). Effects of smoked marijuana on food intake and body weight of humans living in a residential laboratory. Appetite, 11(1), 1–14. https://doi.org/10.1016/s0195-6663(88)80017-5
- Corey-Bloom, J., Wolfson, T., Gamst, A., Jin, S., Marcotte, T. D., Bentley, H., & Gouaux, B. (2012). Smoked cannabis for spasticity in multiple sclerosis: a randomized, placebo-controlled trial. Canadian Medical Association Journal, 184(10), 1143–1150. https://doi.org/10.1503/cmaj.110837
- Kim, K., Moore, D. H., Makriyannis, A., & Abood, M. E. (2006). AM1241, a cannabinoid CB2 receptor selective compound, delays disease progression in a mouse model of amyotrophic lateral sclerosis. European journal of pharmacology, 542(1-3), 100–105. https://doi.org/10.1016/j.ejphar.2006.05.025
- Institute of Medicine (US); Joy JE, Watson SJ Jr., Benson JA Jr., editors. Marijuana and Medicine: Assessing the Science Base. Washington (DC): National Academies Press (US); 1999. 4, The Medical Value of Marijuana and Related Substances. Available from: https://www.ncbi.nlm.nih.gov/books/NBK230711/
- Rosenberg, E. C., Tsien, R. W., Whalley, B. J., & Devinsky, O. (2015). Cannabinoids and Epilepsy. Neurotherapeutics, 12(4), 747–768. https://doi.org/10.1007/s13311-015-0375-5
- Ware, M. A., Wang, T., Shapiro, S., Robinson, A., Ducruet, T., Huynh, T., Gamsa, A., Bennett, G. J., & Collet, J. P. (2010). Smoked cannabis for chronic neuropathic pain: a randomized controlled trial. CMAJ : Canadian Medical Association journal = journal de l’Association medicale canadienne, 182(14), E694–E701. https://doi.org/10.1503/cmaj.091414
- Wang, Z. Y., Wang, P., & Bjorling, D. E. (2014). Treatment with a Cannabinoid Receptor 2 Agonist Decreases Severity of Established Cystitis. Journal of Urology, 191(4), 1153–1158. https://doi.org/10.1016/j.juro.2013.10.102
- Greco, R., Gasperi, V., Maccarrone, M., & Tassorelli, C. (2010). The endocannabinoid system and migraine. Experimental Neurology, 224(1), 85–91. https://doi.org/10.1016/j.expneurol.2010.03.029
- Richardson, D., Pearson, R. G., Kurian, N., Latif, M. L., Garle, M. J., Barrett, D. A., Kendall, D. A., Scammell, B. E., Reeve, A. J., & Chapman, V. (2008). Characterisation of the cannabinoid receptor system in synovial tissue and fluid in patients with osteoarthritis and rheumatoid arthritis. Arthritis research & therapy, 10(2), R43. https://doi.org/10.1186/ar2401
- Kong, Y., Wang, W., Zhang, C., Wu, Y., Liu, Y., & Zhou, X. (2016). Cannabinoid WIN‑55,212‑2 mesylate inhibits ADAMTS‑4 activity in human osteoarthritic articular chondrocytes by inhibiting expression of syndecan‑1. Molecular medicine reports, 13(6), 4569–4576. https://doi.org/10.3892/mmr.2016.5137
- D. R. Blake, P. Robson, M. Ho, R. W. Jubb, C. S. McCabe, Preliminary assessment of the efficacy, tolerability and safety of a cannabis-based medicine (Sativex) in the treatment of pain caused by rheumatoid arthritis, Rheumatology, Volume 45, Issue 1, January 2006, Pages 50–52, https://doi.org/10.1093/rheumatology/kei183
- Fiz, J., Durán, M., Capellà, D., Carbonell, J., & Farré, M. (2011). Cannabis Use in Patients with Fibromyalgia: Effect on Symptoms Relief and Health-Related Quality of Life. PLoS ONE, 6(4), e18440. https://doi.org/10.1371/journal.pone.0018440
- Bab, I., Zimmer, A., & Melamed, E. (2009). Cannabinoids and the skeleton: From marijuana to reversal of bone loss. Annals of Medicine, 41(8), 560–567. https://doi.org/10.1080/07853890903121025
- Silveira, J. W., Issy, A. C., Castania, V. A., Salmon, C. E., Nogueira-Barbosa, M. H., Guimarães, F. S., Defino, H. L., & Del Bel, E. (2014). Protective effects of cannabidiol on lesion-induced intervertebral disc degeneration. PloS one, 9(12), e113161. https://doi.org/10.1371/journal.pone.0113161
- Consroe, P., Sandyk, R., & Snider, S. R. (1986). Open label evaluation of cannabidiol in dystonic movement disorders. International Journal of Neuroscience, 30(4), 277–282. https://doi.org/10.3109/00207458608985678
- Blázquez, C., Chiarlone, A., Sagredo, O., Aguado, T., Pazos, M. R., Resel, E., . . . Guzmán, M. (2010). Loss of striatal type 1 cannabinoid receptors is a key pathogenic factor in Huntington’s disease. Brain, 134(1), 119–136. https://doi.org/10.1093/brain/awq278
- Sieradzan, K., Fox, S., Hill, M., Dick, J., Crossman, A., & Brotchie, J. (2001). Cannabinoids reduce levodopa-induced dyskinesia in Parkinson’s disease: A pilot study. Neurology, 57(11), 2108–2111. https://doi.org/10.1212/wnl.57.11.2108
- Kirsten R. Müller-Vahl, “Treatment of Tourette Syndrome with Cannabinoids“, Behavioural Neurology, vol. 27, Article ID 294264, 6 pages, 2013. https://doi.org/10.3233/BEN-120276
- Tomida, I. (2004). Cannabinoids and glaucoma. British Journal of Ophthalmology, 88(5), 708–713. https://doi.org/10.1136/bjo.2003.032250
- Williams, S. J., Hartley, J. P., & Graham, J. D. (1976). Bronchodilator effect of delta1-tetrahydrocannabinol administered by aerosol of asthmatic patients. Thorax, 31(6), 720–723. https://doi.org/10.1136/thx.31.6.720
- Crawford, W. J., & Merritt, J. C. (1979). Effects of tetrahydrocannabinol on arterial and intraocular hypertension. International journal of clinical pharmacology and biopharmacy, 17(5), 191–196. https://pubmed.ncbi.nlm.nih.gov/468444/
- Bergamaschi, M. M., Queiroz, R. H. C., Chagas, M. H. N., de Oliveira, D. C. G., de Martinis, B. S., Kapczinski, F., . . . Crippa, J. A. S. (2011). Cannabidiol Reduces the Anxiety Induced by Simulated Public Speaking in Treatment-Naïve Social Phobia Patients. Neuropsychopharmacology, 36(6), 1219–1226. https://doi.org/10.1038/npp.2011.6
- Bambico, F. R., Katz, N., Debonnel, G., & Gobbi, G. (2007). Cannabinoids Elicit Antidepressant-Like Behavior and Activate Serotonergic Neurons through the Medial Prefrontal Cortex. Journal of Neuroscience, 27(43), 11700–11711. https://doi.org/10.1523/jneurosci.1636-07.2007
- Russo, E., Guy, G., & Robson, P. (2007). Cannabis, Pain, and Sleep: Lessons from Therapeutic Clinical Trials ofSativex®, a Cannabis-Based Medicine. Chemistry & Biodiversity, 4(8), 1729–1743. https://doi.org/10.1002/cbdv.200790150
- Fraser, G. A. (2009). The Use of a Synthetic Cannabinoid in the Management of Treatment-Resistant Nightmares in Posttraumatic Stress Disorder (PTSD). CNS Neuroscience & Therapeutics, 15(1), 84–88. https://doi.org/10.1111/j.1755-5949.2008.00071.x
- Reiman, A. Cannabis as a substitute for alcohol and other drugs. Harm Reduct J 6, 35 (2009). https://doi.org/10.1186/1477-7517-6-35
- Leweke, F. M., Piomelli, D., Pahlisch, F., Muhl, D., Gerth, C. W., Hoyer, C., . . . Koethe, D. (2012). Cannabidiol enhances anandamide signaling and alleviates psychotic symptoms of schizophrenia. Translational Psychiatry, 2(3), e94. https://doi.org/10.1038/tp.2012.15
- Eubanks, L. M., Rogers, C. J., Beuscher, Koob, G. F., Olson, A. J., Dickerson, T. J., & Janda, K. D. (2006). A Molecular Link between the Active Component of Marijuana and Alzheimer’s Disease Pathology. Molecular Pharmaceutics, 3(6), 773–777. https://doi.org/10.1021/mp060066m
- Dvorak, M., Watkinson, A., McGlone, F., & Rukwied, R. (2003). Histamine induced responses are attenuated by a cannabinoid receptor agonist in human skin. Inflammation Research, 52(6), 238–245. https://doi.org/10.1007/s00011-003-1162-z
- Wong, B. S., Camilleri, M., Busciglio, I., Carlson, P., Szarka, L. A., Burton, D., & Zinsmeister, A. R. (2011). Pharmacogenetic Trial of a Cannabinoid Agonist Shows Reduced Fasting Colonic Motility in Patients With Nonconstipated Irritable Bowel Syndrome. Gastroenterology, 141(5), 1638–1647.e7. https://doi.org/10.1053/j.gastro.2011.07.036
- Naftali, T., Lev, L. B., Yablecovitch, D., Half, E., & Konikoff, F. M. (2011). Treatment of Crohn’s disease with cannabis: an observational study. The Israel Medical Association journal : IMAJ, 13(8), 455–458. https://pubmed.ncbi.nlm.nih.gov/21910367/
- Lim, M. P., Devi, L. A., & Rozenfeld, R. (2011). Cannabidiol causes activated hepatic stellate cell death through a mechanism of endoplasmic reticulum stress-induced apoptosis. Cell Death & Disease, 2(6), e170. https://doi.org/10.1038/cddis.2011.52
- Levendal, R. A., Schumann, D., Donath, M., & Frost, C. (2012). Cannabis exposure associated with weight reduction and β-cell protection in an obese rat model. Phytomedicine, 19(7), 575–582. https://doi.org/10.1016/j.phymed.2012.02.001
- Rajavashisth, T. B., Shaheen, M., Norris, K. C., Pan, D., Sinha, S. K., Ortega, J., & Friedman, T. C. (2012). Decreased prevalence of diabetes in marijuana users: cross-sectional data from the National Health and Nutrition Examination Survey (NHANES) III. BMJ Open, 2(1), e000494. https://doi.org/10.1136/bmjopen-2011-000494
- Scott, K. A., Dalgleish, A. G., & Liu, W. M. (2014). The Combination of Cannabidiol and Δ9-Tetrahydrocannabinol Enhances the Anticancer Effects of Radiation in an Orthotopic Murine Glioma Model. Molecular Cancer Therapeutics, 13(12), 2955–2967. https://doi.org/10.1158/1535-7163.mct-14-0402
- Elbaz, M., Nasser, M. W., Ravi, J., Wani, N. A., Ahirwar, D. K., Zhao, H., Oghumu, S., Satoskar, A. R., Shilo, K., Carson, W. E., 3rd, & Ganju, R. K. (2015). Modulation of the tumor microenvironment and inhibition of EGF/EGFR pathway: novel anti-tumor mechanisms of Cannabidiol in breast cancer. Molecular oncology, 9(4), 906–919. https://doi.org/10.1016/j.molonc.2014.12.010
- Adinolfi, B., Romanini, A., Vanni, A., Martinotti, E., Chicca, A., Fogli, S., & Nieri, P. (2013). Anticancer activity of anandamide in human cutaneous melanoma cells. European Journal of Pharmacology, 718(1–3), 154–159. https://doi.org/10.1016/j.ejphar.2013.08.039
- Thomas, A. A., Wallner, L. P., Quinn, V. P., Slezak, J., van den Eeden, S. K., Chien, G. W., & Jacobsen, S. J. (2015). Association Between Cannabis Use and the Risk of Bladder Cancer: Results From the California Men’s Health Study. Urology, 85(2), 388–393. https://doi.org/10.1016/j.urology.2014.08.060
- Scott, K. A., Shah, S., Dalgleish, A. G., & Liu, W. M. (2013). Enhancing the activity of cannabidiol and other cannabinoids in vitro through modifications to drug combinations and treatment schedules. Anticancer research, 33(10), 4373–4380. https://pubmed.ncbi.nlm.nih.gov/24123005/
- Haustein, M., Ramer, R., Linnebacher, M., Manda, K., & Hinz, B. (2014). Cannabinoids increase lung cancer cell lysis by lymphokine-activated killer cells via upregulation of ICAM-1. Biochemical Pharmacology, 92(2), 312–325. https://doi.org/10.1016/j.bcp.2014.07.014
- Carracedo, A., Gironella, M., Lorente, M., Garcia, S., Guzmán, M., Velasco, G., & Iovanna, J. L. (2006). Cannabinoids Induce Apoptosis of Pancreatic Tumor Cells via Endoplasmic Reticulum Stress–Related Genes. Cancer Research, 66(13), 6748–6755. https://doi.org/10.1158/0008-5472.can-06-0169
- Aviello, G., Romano, B., Borrelli, F., Capasso, R., Gallo, L., Piscitelli, F., . . . Izzo, A. A. (2012). Chemopreventive effect of the non-psychotropic phytocannabinoid cannabidiol on experimental colon cancer. Journal of Molecular Medicine, 90(8), 925–934. https://doi.org/10.1007/s00109-011-0856-x
- Olea-Herrero, N., Vara, D., Malagarie-Cazenave, S., & Díaz-Laviada, I. (2009). Inhibition of human tumour prostate PC-3 cell growth by cannabinoids R(+)-Methanandamide and JWH-015: Involvement of CB2. British Journal of Cancer, 101(6), 940–950. https://doi.org/10.1038/sj.bjc.6605248
- Deiana, S., Watanabe, A., Yamasaki, Y., Amada, N., Arthur, M., Fleming, S., . . . Riedel, G. (2011). Plasma and brain pharmacokinetic profile of cannabidiol (CBD), cannabidivarine (CBDV), Δ9-tetrahydrocannabivarin (THCV) and cannabigerol (CBG) in rats and mice following oral and intraperitoneal administration and CBD action on obsessive–compulsive behaviour. Psychopharmacology, 219(3), 859–873. https://doi.org/10.1007/s00213-011-2415-0
- Steffens, S., Veillard, N. R., Arnaud, C., Pelli, G., Burger, F., Staub, C., Karsak, M., Zimmer, A., Frossard, J. L., & Mach, F. (2005). Low dose oral cannabinoid therapy reduces progression of atherosclerosis in mice. Nature, 434(7034), 782–786. https://doi.org/10.1038/nature03389
- Campos, A. C., Ortega, Z., Palazuelos, J., Fogaça, M. V., Aguiar, D. C., Díaz-Alonso, J., . . . Guimarães, F. S. (2013). The anxiolytic effect of cannabidiol on chronically stressed mice depends on hippocampal neurogenesis: involvement of the endocannabinoid system. International Journal of Neuropsychopharmacology, 16(6), 1407–1419. https://doi.org/10.1017/s1461145712001502
- Nguyen, B. M., Kim, D., Bricker, S., Bongard, F., Neville, A., Putnam, B., . . . Plurad, D. (2014). Effect of Marijuana Use on Outcomes in Traumatic Brain Injury. The American Surgeon, 80(10), 979–983. https://doi.org/10.1177/000313481408001015
- Milz E, Grotenhermen F. Successful Therapy of Treatment Resistant Adult ADHD with Cannabis: Experience from a Medical Practice with 30 Patients. Abstract Book of the International Cannabinoid in Medicine & Research Conference 2015 in Sestri Levante (GE); Italy. 2015; p. 85. Google Scholar
- Abush, H., & Akirav, I. (2013). Cannabinoids Ameliorate Impairments Induced by Chronic Stress to Synaptic Plasticity and Short-Term Memory. Neuropsychopharmacology, 38(8), 1521–1534. https://doi.org/10.1038/npp.2013.51
- Liao, Y., Bin, J., Luo, T., Zhao, H., Ledent, C., Asakura, M., . . . Kitakaze, M. (2013). CB1 cannabinoid receptor deficiency promotes cardiac remodeling induced by pressure overload in mice. International Journal of Cardiology, 167(5), 1936–1944. https://doi.org/10.1016/j.ijcard.2012.05.033
- Campos, A., Brant, F., Miranda, A., Machado, F., & Teixeira, A. (2015). Cannabidiol increases survival and promotes rescue of cognitive function in a murine model of cerebral malaria. Neuroscience, 289, 166–180. https://doi.org/10.1016/j.neuroscience.2014.12.051
- Chowdhury A. R. (1987). Effect of pharmacological agents on male reproduction. Advances in contraceptive delivery systems : CDS, 3(4), 347–352. https://pubmed.ncbi.nlm.nih.gov/12341906/
- Lynn, B. K., López, J. D., Miller, C., Thompson, J., & Campian, E. C. (2019). The Relationship between Marijuana Use Prior to Sex and Sexual Function in Women. Sexual medicine, 7(2), 192–197. https://doi.org/10.1016/j.esxm.2019.01.003
- Lancz, G., Specter, S., & Brown, H. K. (1991). Suppressive Effect of -9-Tetrahydrocannabinol on Herpes Simplex Virus Infectivity In Vitro. Experimental Biology and Medicine, 196(4), 401–404. https://doi.org/10.3181/00379727-196-43206
- Green, B., Kavanagh, D., & Young, R. (2003). Being stoned: a review of self-reported cannabis effects. Drug and alcohol review, 22(4), 453–460. https://doi.org/10.1080/09595230310001613976
- Mark Anderson, D., Hansen, B., & Rees, D. I. (2013). Medical Marijuana Laws, Traffic Fatalities, and Alcohol Consumption. The Journal of Law and Economics, 56(2), 333–369. https://doi.org/10.1086/668812
- Morris, R. G., TenEyck, M., Barnes, J. C., & Kovandzic, T. V. (2014). The Effect of Medical Marijuana Laws on Crime: Evidence from State Panel Data, 1990–2006. PLoS ONE, 9(3), e92816. https://doi.org/10.1371/journal.pone.0092816
- Jones, K. A., Blagrove, M., & Parrott, A. C. (2009). Cannabis and Ecstasy/MDMA: Empirical Measures of Creativity in Recreational Users. Journal of Psychoactive Drugs, 41(4), 323–329. https://doi.org/10.1080/02791072.2009.10399769
- Lachenmeier, D. W., & Rehm, J. (2015). Comparative risk assessment of alcohol, tobacco, cannabis and other illicit drugs using the margin of exposure approach. Scientific Reports, 5(1). https://doi.org/10.1038/srep08126
- Morgan, C. J., Das, R. K., Joye, A., Curran, H. V., & Kamboj, S. K. (2013). Cannabidiol reduces cigarette consumption in tobacco smokers: Preliminary findings. Addictive Behaviors, 38(9), 2433–2436. https://doi.org/10.1016/j.addbeh.2013.03.011
- Colorado Center On Law & Policy, & Stiffler, C. (2012). Amendment 64 would produce $60 million in new revenue and savings for Colorado. Colorado Center On Law & Policy. Retrieved from https://cclponline.org/wp-content/uploads/2013/11/amendment_64_analysis_final.pdf
- Moran, Thomas. (2011). Just a Little Bit of History Repeating: The California Model of Marijuana Legalization and How it Might Affect Racial and Ethnic Minorities. https://scholarlycommons.law.wlu.edu/crsj/vol17/iss2/8/